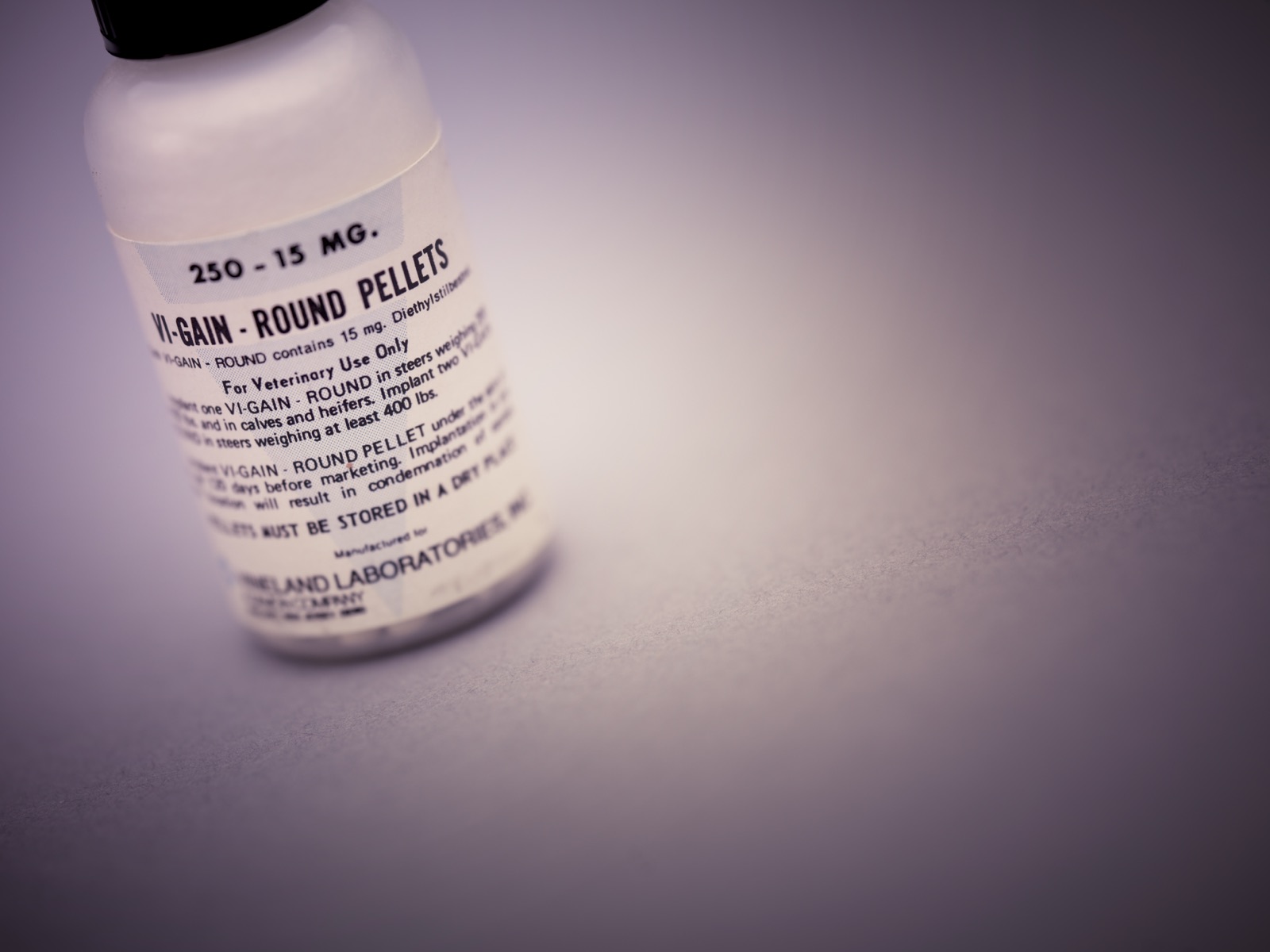
A bottle of diethylstilbestrol (DES) — this one a veterinary product, growth-promoting implant pellets for cattle. The same synthetic estrogen, in tablet form, was prescribed to millions of pregnant women to prevent miscarriage. That a single drug could be both a livestock growth-promoter and a treatment for human pregnancy hints at how loosely its powers were understood. Wikimedia Commons / U.S. Food and Drug Administration, Public domain.
DES and the Cancer That Waited a Generation
United States and beyond, 1940–1971 — a synthetic hormone was prescribed to millions of pregnant women to prevent miscarriage. It did not work, and a study had said so by 1953. Twenty years later, the daughters who had been exposed in the womb began developing a cancer almost unknown in the young
- Category
- Health & Medicine
- Published
- Length
- 4,240 words · 19 min read
- Author
- The editors
The DES story sits alongside thalidomide as one of the two great pharmaceutical disasters that reshaped how the world thinks about drugs and pregnancy — but it is, in a way, the more insidious of the two. Thalidomide's harm was visible at birth and unmistakable. DES's harm was invisible for two decades, hidden inside healthy-seeming babies who would not learn what had been done to them until they were grown. It is a story about the hardest kind of damage to detect: the kind that waits.
This is the story of that waiting, and of what finally surfaced.
The wonder hormone
DES was born of a genuine scientific achievement. In 1938 the British biochemist Edward Charles Dodds synthesised the first potent estrogen that did not have to be extracted from animals — a cheap, orally active synthetic hormone that could be manufactured in quantity. Crucially, Dodds and his institution did not patent it, a decision often described as high-minded; the practical result was that any pharmaceutical company could make and sell DES, and many did. There was no single manufacturer with a monopoly, a brand to protect, or sole responsibility — a fact that would matter enormously decades later.
The drug arrived in an age intoxicated by hormones. The 1930s and 1940s had seen estrogen and the other sex hormones isolated and understood for the first time, and medicine was giddy with the possibilities — hormones seemed like master switches for the body, capable of fixing whatever ailed it. Into this enthusiasm came two influential Harvard physicians, George and Olive Smith, who developed and promoted a theory that miscarriage was caused by faltering hormone levels and that DES, by boosting them, could sustain a pregnancy. They published dosing schedules, lectured, and lent the prestige of a great medical school to the idea. Their advocacy, more than any single company's marketing, helped turn DES into a routine part of prenatal care. The theory was elegant, authoritative, and wrong — but it came clothed in the confidence of the era's leading science, which is exactly why it was so hard, later, to dislodge.

Estrogen was understood to be central to pregnancy, and a plausible — though, as it turned out, mistaken — theory held that miscarriages and complications were caused by a deficiency of it. Giving pregnant women extra estrogen in the form of DES therefore seemed a reasonable way to support a faltering pregnancy. From the early 1940s, DES was promoted for exactly this: to prevent miscarriage, premature birth, and other complications, and increasingly not just for women with a history of problems but as a general tonic for pregnancy. Advertisements urged its use to make pregnancies safer and even, in the notorious phrasing of the time, to produce "bigger and stronger babies." Millions of prescriptions were written. The drug was woven into ordinary prenatal care.
The marketing did its work on doctors and mothers alike. DES was advertised in medical journals as a way to make pregnancy safer and its outcomes better, with little of the caution such claims deserved, and it was prescribed not only to women who had suffered miscarriages but, in many cases, prophylactically — to women with no particular problem at all, on the theory that it could only help. That breadth of use is what turned DES from a niche treatment into a mass exposure: a drug given to large numbers of essentially healthy pregnant women, multiplying the population that would later be put at risk. The reassurance was total and the evidence was thin, a combination that recurs in nearly every pharmaceutical disaster — the confident promise outrunning the proof, with the gap between them filled, eventually, by the people who were harmed.
It did not even work
The most damning fact about DES is not merely that it was dangerous, but that it was useless for the purpose it was sold for — and that this was known, in good time, and ignored. In 1953, researchers at the University of Chicago published a large, well-designed controlled trial comparing DES against a placebo in pregnant women. The result was clear: DES did nothing to prevent miscarriage or premature birth. It simply did not work.
In a rational system, that should have ended DES's use in pregnancy on the spot. It did not. Habit, marketing, the momentum of an established prescription, and the simple difficulty of un-teaching doctors something they already believed kept DES flowing to pregnant women for nearly twenty more years. This is the part of the story that is easy to skip past but should not be: the disaster that followed was not only the result of a hidden danger. It was compounded by the continued use of a drug that the medical literature had already shown to be worthless for its stated purpose. The women who took DES after 1953, and the children harmed, were exposed to a risk that bought them nothing at all.
There is a lesson here about how medicine actually changes its mind, and how slowly. A single well-designed negative study, however rigorous, rarely overturns an established practice on its own; the belief that DES helped was held by respected authorities, reinforced by the natural human tendency to credit a drug when a pregnancy went well and to blame bad luck when it did not. Every doctor who had prescribed DES and seen a healthy baby born felt confirmed in the decision, even though the baby would almost certainly have been born without it. This is the trap of treating a condition that usually resolves on its own: the treatment gets the credit for outcomes it had nothing to do with, and no amount of contrary data quite dislodges the impression of success. DES rode that illusion for two decades after the evidence had turned against it.
The harm that skipped a generation
For a long time, DES seemed to do no obvious damage. The women who took it were largely fine; their pregnancies proceeded; their babies were born looking healthy. Whatever DES was doing, it was not leaving a mark anyone could see. The catastrophe was developing silently, in the bodies of the daughters, and it would take until those daughters reached adolescence and early adulthood to reveal itself.
In 1971, a team of doctors led by Arthur Herbst published a study that connected the dots. They had been confronted by something that should not have existed: a cluster of young women, teenagers and women in their early twenties, with clear cell adenocarcinoma of the vagina and cervix — a cancer so rare in the young as to be almost unheard of. Searching for what these patients had in common, the investigators found it not in the patients themselves but in their mothers: the affected young women had been exposed, before birth, to DES taken by their mothers during pregnancy. The drug had crossed the placenta two decades earlier and altered the developing reproductive tract in ways that, much later, could turn cancerous. It was a landmark and a horror at once — the first demonstration that a drug could act as a "transplacental carcinogen," causing cancer not in the person who swallowed it but in the child they were carrying, a generation removed.
The discovery owed as much to detective work as to medicine. Clear cell adenocarcinoma was so vanishingly rare in young women that even a handful of cases appearing in the same place and time was an anomaly worth chasing, and it was the mother of one patient who reportedly first raised the possibility that the DES she had taken might be to blame. Tracing the connection meant going back two decades into the medical histories of the mothers, not the patients — an unusual direction for cancer research, which looks for causes in the life of the person who is ill, not in a pill swallowed by someone else before they were born. The finding's implications rippled outward immediately: if DES could do this, then the whole exposed generation — millions of people who had no idea they had been exposed to anything — was potentially at risk, and needed to be found, informed, and monitored. A private medical tragedy became, overnight, a public-health problem of enormous scale.
The wider damage
The cancer was the most dramatic harm, but it was also, mercifully, relatively rare; the broader damage was wider and quieter. DES daughters, as the exposed generation came to be called, suffered a range of injuries to the reproductive system: structural abnormalities of the uterus, cervix, and vagina; higher rates of infertility; and, for those who could conceive, sharply increased risks of miscarriage, ectopic pregnancy, and premature birth — the very outcomes the drug had been sold to prevent, now inflicted on the next generation. DES sons, too, showed elevated rates of genital abnormalities. And the women who had originally taken DES carried their own modestly raised risk of breast cancer. A drug given to make pregnancy safer had, across the generations, made it more dangerous, and had reached into the bodies of children who never took it.
The other uses
DES's history is made stranger, and its dangers underlined, by how many other things the same drug was used for. Because it was a cheap, powerful synthetic estrogen, DES was pressed into service across medicine and agriculture. It was given to suppress lactation, to treat prostate cancer in men, and as a high-dose "morning-after" contraceptive. It was used, chillingly, as a form of chemical castration — the British mathematician Alan Turing was subjected to DES injections in 1952 as a court-ordered "treatment" for homosexuality, with devastating effects. And on a vast scale, DES was fed and implanted into livestock as a growth promoter, to fatten cattle and poultry faster — the use shown on the bottle that opens this article.

The agricultural use eventually triggered its own slow-motion ban, as concern grew that DES residues in meat could be carcinogenic to the people who ate it. That a single synthetic hormone could be deployed to prevent human miscarriage, fatten steers, suppress milk, dose prisoners, and chemically castrate a gay man — all on the same loose confidence in a powerful drug only partly understood — is the most revealing fact about the medical culture that produced the DES disaster. The drug was treated as a versatile tool. Its capacity to cause profound, delayed harm was simply not part of the calculation.
The reckoning
In 1971, the same year the cancer link was published, the United States Food and Drug Administration advised that DES should no longer be used in pregnancy. The immediate medical question was settled. But for the women who had been harmed, the harder reckoning — holding someone accountable — ran into an obstacle peculiar to DES, and it produced one of the most important innovations in the history of American injury law.

The problem was this: DES had been manufactured by many different companies, all selling essentially the same generic drug, and a woman who developed cancer in the 1970s from a pill her mother had taken in the 1950s usually had no way of knowing which company had made that particular pill. Under traditional law, a plaintiff who cannot prove which defendant caused her injury cannot recover at all — meaning the very ubiquity of DES, the fact that so many firms had made it, would have let all of them escape. In 1980, in the case of Sindell v. Abbott Laboratories, the California Supreme Court refused to accept that outcome. It created the doctrine of "market-share liability": where a plaintiff cannot identify the specific manufacturer of a fungible product that harmed her, the makers can be held liable in proportion to their share of the market. It was a genuine innovation, controversial and influential, and DES was its origin.
The litigation went on for years and brought some compensation to some of those harmed, though as with every such reckoning it was partial, slow, and never commensurate with the damage. Advocacy groups of DES daughters and sons formed, pressed for research and recognition, and pushed public-health authorities to track the exposed population — work that continues, because the health effects of DES exposure have unfolded across a lifetime and may yet reach into a third generation, the grandchildren of the women who first took the pills.
This is part of what makes DES so difficult to close the book on. Most disasters have an end — a settlement signed, a drug withdrawn, a generation that ages out of the danger. DES does not, quite. Because its effects were written into developing bodies, they continue to play out across the lifespans of the exposed, who are now elderly, and may extend to descendants who never came near the drug. Public- health agencies still maintain DES exposure registries and advise those who may have been exposed to inform their doctors. Many people carry the risk without knowing it, because the prescriptions were written so long ago, often without explanation, to mothers who are no longer alive to be asked. The disaster has no clean expiry date; it simply thins out across time, a long tail of consequence trailing from pills swallowed three-quarters of a century ago.
What is established, and what it means
There is no factual dispute at the centre of the DES story. The drug was given to pregnant women; it did not prevent miscarriage; it caused cancer and other harms in the children exposed in the womb; the link was established in 1971; the law responded in 1980. What DES offers is not a mystery but a set of hard lessons, and they are worth naming plainly.
The first is about evidence. DES was prescribed for a purpose it did not serve, and kept in use for nearly two decades after a good study said so. The harm it caused was real, but the exposure that led to that harm was, in a sense, gratuitous — undertaken for a benefit that did not exist. The second lesson is about time. DES is the textbook case of latency: a drug can appear completely safe for twenty years and then reveal a catastrophe, because the damage was done to a developing body that had not yet grown into the disease. That possibility — that harm can hide for a generation — is one of the deepest reasons modern drug testing is as cautious, and as slow, as it is, especially around pregnancy. The third lesson is structural: when a dangerous product is made by everyone and traceable to no one, ordinary accountability can fail entirely, and the law has to be remade to cope.
In the end, DES is a story about the limits of seeing. For thirty years it looked like a helpful, even gentle, drug — recommended by trusted doctors, taken by careful mothers, producing healthy babies. Everything visible said it was fine. The truth was that it had quietly rewritten the futures of the children exposed to it, and that truth would not show itself until those children were grown and a strange cancer forced someone to look. The drug taught medicine that safety cannot always be read in the present tense — that a pill can be judged harmless by everyone who can see, and still be doing harm that only the next generation will feel. The women and men who carry DES in their histories are the proof, and the warning, that some damage keeps its own slow time.
Sources
- A. L. Herbst, H. Ulfelder, and D. C. Poskanzer, "Adenocarcinoma of the Vagina: Association of Maternal Stilbestrol Therapy with Tumor Appearance in Young Women," New England Journal of Medicine (1971) — primary.
- W. J. Dieckmann et al., the 1953 University of Chicago controlled trial finding DES ineffective in pregnancy — primary.
- Sindell v. Abbott Laboratories, California Supreme Court (1980) — primary.
- US Food and Drug Administration advisory against DES use in pregnancy (1971) and subsequent guidance — primary.
- Centers for Disease Control and Prevention, DES follow-up studies and resources on DES exposure — secondary/academic.
- Susan E. Bell, DES Daughters: Embodied Knowledge and the Transformation of Women's Health Politics (2009) — academic.
- Robert Meyers, D.E.S.: The Bitter Pill (1983) — secondary.
- Histories of DES, transplacental carcinogenesis, and reproductive toxicology — academic.
- Accounts of DES's other uses, including livestock growth promotion and the chemical castration of Alan Turing — secondary.
Inspired this / based on it
Judith Helfand
A DES daughter's first-person documentary about her own DES-related cancer and her family.
Susan E. Bell
Temple University Press. A study of the DES daughters and the women's-health movement.
Robert Meyers
An early popular account of the DES disaster.
Filed under
- #des-pregnancy
- #diethylstilbestrol
- #pharmaceuticals
- #birth-defects
- #cancer
- #drug-safety
- #market-share-liability
- #medical-ethics
- #1950s
- #1970s
- #confirmed
Click any tag for every article carrying it.
Continue reading

Thalidomide and the Wonder Drug That Came for the Unborn
It was sold as the safest drug imaginable. Thalidomide — marketed as Contergan in West Germany, Distaval in Britain, Neurosedyn in Sweden, and Kevadon in North America — was a sedative and sleeping pill that the German company Grünenthal advertised as so harmless it was impossible to take a fatal overdose, suitable even for children, and, crucially, safe for pregnant women suffering morning sickness. None of it had been properly tested for what it did to a developing fetus, because in the late 1950s almost no one tested for that at all. Between 1957 and 1961 the drug was sold in dozens of countries, and as it spread, something terrible began to appear in maternity wards: babies born with limbs shortened or missing entirely — hands attached at the shoulder, the condition doctors called phocomelia — along with damage to ears, eyes, hearts, and internal organs. By the time the cause was identified and the drug pulled from shelves in late 1961, roughly ten thousand children worldwide had been born with thalidomide injuries, and thousands more had died before or shortly after birth. The United States was very nearly spared entirely, because of one woman: Frances Oldham Kelsey, a new reviewer at the Food and Drug Administration who, against sustained pressure from the manufacturer, simply refused to approve it. The thalidomide disaster destroyed the comfortable assumption that a drug on the market must be safe, broke the makers' long resistance to accountability, and forced governments to rebuild the entire system by which medicines are tested and approved. This is the story of how it happened, who stopped it, and what it changed.

DuPont and PFOA
In October 1998, a West Virginia cattle farmer named Wilbur Tennant called a Cincinnati lawyer named Robert Bilott about 153 dead cows. The cows had been drinking from Dry Run Creek, three miles downstream from the DuPont Washington Works chemical plant. Tennant's home video showed cattle with bloody mouths, gum cancer, and stumbling gaits before they died. Bilott — a corporate-defense attorney at Taft Stettinius & Hollister who had spent his career representing chemical companies — agreed to look at the file as a personal favor to his grandmother, who knew the Tennant family. The look became a twenty-year case. By the time Bilott was finished, he had uncovered: that DuPont had been releasing perfluorooctanoic acid (PFOA, code-named 'C8') into the Ohio River and into landfills for over forty years; that DuPont had known PFOA was toxic since at least 1961; that the company's own animal studies in 1981 had shown birth defects in offspring of exposed female workers; and that approximately 99% of the U.S. population, by 2007, had detectable levels of PFOA in their blood. The 2005 EPA fine ($16.5 million) was the largest in U.S. environmental enforcement history at the time. The 2017 multi-district settlement was $670.7 million. The C8 Science Panel — established as part of an earlier 2005 class-action settlement — confirmed by 2012 that PFOA is causally linked to six diseases including kidney and testicular cancer. PFOA was phased out of U.S. production by 2015. Its environmental persistence — half-life in human blood is approximately 3.8 years — means that, by 2025, every American adult has some PFOA exposure dating from the production era. The chemical that made non-stick cookware possible is, in this sense, still with us.

Big Tobacco's Cancer Cover-Up
On the morning of January 4, 1954, a full-page advertisement appeared in 448 American newspapers under the headline *A Frank Statement to Cigarette Smokers*. It was signed by the chief executives of the United States' six largest tobacco companies. The advertisement assured the American public that 'there is no proof that cigarette smoking is one of the causes of cancer' and that the industry would underwrite scientific research to find the truth. The advertisement had been drafted by John W. Hill of the Hill & Knowlton public-relations firm, hired by the tobacco industry's chief executives at a meeting at the Plaza Hotel in New York on December 14-15, 1953. The strategy that the meeting produced — manufacture doubt about epidemiological evidence the industry already privately accepted, do this through industry-funded research that produced findings inconsistent with the public-health consensus, and continue to sell cigarettes to American smokers while doing so — would be sustained for forty-four years. It would be ended, in 1998, by the Master Settlement Agreement: the largest civil legal settlement in American history at $206 billion across 25 years, paid by the surviving tobacco companies to 46 states, the District of Columbia, and five U.S. territories. By that point, an estimated 8 million Americans had died from smoking-related cancers, cardiovascular disease, and respiratory illness during the cover-up period.