
A 1960 bottle of Kevadon — thalidomide — distributed in the United States by the Wm. S. Merrell Company under an 'investigational use' label while the firm sought approval that the FDA never granted. Elsewhere it was sold freely as Contergan, Distaval, and Neurosedyn, and marketed as safe enough for pregnant women. Wikimedia Commons / U.S. Food and Drug Administration, Public domain.
Thalidomide and the Wonder Drug That Came for the Unborn
Germany, Britain, Sweden, and beyond, 1957–1962 — a sedative sold as so safe it was given to pregnant women for morning sickness instead caused some ten thousand children to be born with devastating malformations. One drug reviewer's refusal spared the United States, and remade how the world tests medicines
- Category
- Health & Medicine
- Published
- Length
- 4,350 words · 20 min read
- Author
- The editors
The thalidomide story is usually told as a tragedy, and it is one. But it is also, unusually, a story with a clear villain's failure and a clear hero's stand, and a genuine turning point: the moment when the modern world decided that a drug must be proven safe before it is sold, rather than presumed safe until it kills. Almost every protection a patient now relies on — the testing, the trials, the warnings, the regulators with the power to say no — exists in something like its current form because of what thalidomide did to a generation of children. That is a high price for a lesson, and the people who paid it did not volunteer.
This is the story of the drug, the disaster, and the reckoning.
The wonder drug
Grünenthal, a pharmaceutical company in the German town of Stolberg, brought thalidomide to market in West Germany in 1957, under the brand name Contergan. It was promoted as a sedative and sleeping aid with a remarkable safety profile: non-toxic, non- addictive, and — the claim that would prove monstrous — impossible to overdose on, so gentle it could be given to children and to pregnant women. In an age newly enamoured of pharmaceutical solutions to everyday discomfort, a safe sleeping pill that also calmed anxiety and quieted the nausea of early pregnancy was a commercial triumph. It sold enormously.
In West Germany, where it had begun, thalidomide was for a time available without prescription — an ordinary household remedy, bought over the counter like aspirin and kept in the medicine cabinet for restless nights and frayed nerves. Grünenthal marketed it aggressively and across a widening range of uses, packaging it into dozens of combination products for coughs, colds, headaches, and the everyday complaints of family life. This ubiquity was part of what made the coming disaster so wide: the drug was not a rare specialist prescription but a mass-market staple, woven into ordinary medicine, and reaching a vast number of people who took it casually for minor troubles — including women in the first uncertain weeks of a pregnancy they might not yet have confirmed.

The reassurance about safety rested on remarkably little. The drug had been tested for the dose that would kill an adult animal — and, strikingly, it seemed almost impossible to find one, which was read as proof of its harmlessness. But it had not been meaningfully tested for what it might do to an embryo, because the reigning assumption of the era was that the placenta acted as a barrier protecting the fetus from drugs the mother took. That assumption was wrong, and thalidomide would be the catastrophe that disproved it. Within a few years the drug had been licensed to companies around the world and sold, under one brand or another, in dozens of countries.
Neurosedyn, Contergan, and the morning-sickness market
The detail that turned a dangerous drug into a generational catastrophe was its marketing to pregnant women. Morning sickness — the nausea and vomiting of early pregnancy — is miserable and common, and a pill advertised as completely safe that could settle it was bound to be widely taken by exactly the population most vulnerable to it. And the vulnerability was cruelly specific. Thalidomide does its damage in a narrow window of early pregnancy, roughly the third to eighth week after conception, when the limbs and organs are forming — often before a woman even knows for certain that she is pregnant. A few tablets taken for nausea during those weeks could be enough.
The results, when they came, were unmistakable and terrible. Babies were born with phocomelia — limbs drastically foreshortened or absent, hands and feet emerging close to the trunk — and with a range of other injuries: malformed or missing ears and deafness, eye defects, damaged hearts, kidneys, and digestive tracts. The pattern was so unusual that doctors who had never seen a single case of such limb defects in their careers were suddenly seeing many. Something was loose in the world, and at first no one knew what. Phocomelia had been so rare that many doctors had only read of it in old textbooks; now clinics in Germany were recording dozens, then hundreds of cases, and similar clusters were appearing in Britain, Sweden, Japan, and elsewhere. The early explanations reached for the anxieties of the age: radioactive fallout from nuclear testing, something in the food supply, a virus, a new chemical in the environment. Because the affected babies were scattered across different countries and the drug hid behind different brand names, no single doctor could easily see the whole picture, and the cause that linked them — a common pill taken weeks earlier, often forgotten by the time the child was born — was precisely the kind of clue most likely to be missed. It took a particular sort of detective work, comparing case after case, to notice that the one thing these mothers shared was a sedative.
The woman who said no
While Europe filled with thalidomide, the United States very nearly escaped, and the reason was a single civil servant doing her job against pressure. In 1960 the Merrell company applied to the FDA for approval to sell thalidomide in America as Kevadon, expecting a formality. The application landed on the desk of Frances Oldham Kelsey, a physician and pharmacologist newly arrived at the agency.

Kelsey was not satisfied. The data on the drug's safety struck her as thin, and she was troubled by reports from Britain of patients developing peripheral neuritis — a painful nerve condition — after long-term use. If the drug could damage an adult's nerves, she reasoned, what might it do to a fetus, about which there was no data at all? She asked Merrell for more evidence. The company pushed back, repeatedly and with mounting frustration, lobbying her superiors and complaining of delay; for them, every month of hold-up was lost money. Kelsey held firm, requesting again and again the studies that did not exist. She refused, in essence, to approve a drug that had not been proven safe. While she stalled, through 1961, the catastrophe in Europe became visible, and the link to thalidomide emerged. The application was never granted. The United States was spared the worst — not by luck, and not by its system working automatically, but by one reviewer willing to be the obstacle.
The escape was not quite total, and the gap is itself revealing. While the application sat unapproved, Merrell had distributed thalidomide to American doctors in enormous quantities as "investigational" samples — a practice then loosely regulated — so that more than a thousand physicians handed the drug to many thousands of patients, some of them pregnant, in what was nominally research but functioned as marketing. A small number of American children were injured as a result. That this happened even with the formal approval withheld shows how porous the old system was, and how close the United States came: had Kelsey been less stubborn, or the European warnings arrived a few months later, the samples would have become a licence and the American toll would have rivalled Europe's. The country was saved by a margin measured in one person's willingness to keep saying no.
Lenz, McBride, and the reckoning of 1961
In Europe and Australia, doctors were converging on the cause. In Germany, the paediatrician and geneticist Widukind Lenz gathered case after case and came to suspect thalidomide; in November 1961 he voiced his suspicion publicly and warned Grünenthal. In Australia, the obstetrician William McBride independently reached the same conclusion, set out in a short letter to the journal The Lancet in December 1961. The drug was the common thread linking mothers of deformed babies who otherwise had nothing in common.
Grünenthal, which had received warning signs and complaints for some time, resisted — disputing the connection, defending its product — but the evidence was overwhelming, and at the end of November 1961 the drug was withdrawn in Germany, with Britain and other countries following within weeks. The withdrawal stopped new cases, but it came years too late for the thousands already born and the thousands already lost. And the question of why a drug had been sold to pregnant women on the strength of a safety claim no one had verified now demanded an answer.
The answer, when it was pieced together, was not flattering to the manufacturer. Grünenthal had been receiving reports of a serious side effect — peripheral neuritis, the nerve damage that had also troubled Kelsey — for a considerable time before the birth-defect crisis, and had tended to minimise and contest such warnings rather than act on them. As cases of malformation began to surface and suspicion turned toward the drug, the company's instinct was to defend its product and question the evidence. Months passed between the first serious warnings and the withdrawal — months in which the drug stayed on shelves and pregnant women kept taking it. Whether that delay is best described as negligence or as something worse was exactly what the later legal reckoning tried, and largely failed, to resolve. What is clear is that the warning signs were there to be heeded before the catastrophe reached its full size, and were not.
Why it was missed — and the chirality myth
Part of the horror of thalidomide is how avoidable it now looks, and part of its scientific legacy is a cautionary tale that is often told slightly wrong. Thalidomide is a "chiral" molecule: it exists in two mirror-image forms, or enantiomers, like a left and a right hand. It became a famous teaching example with a tidy moral — that one enantiomer was the helpful sedative and the other the teratogen that maimed the fetus, so that a purer drug might have been safe.
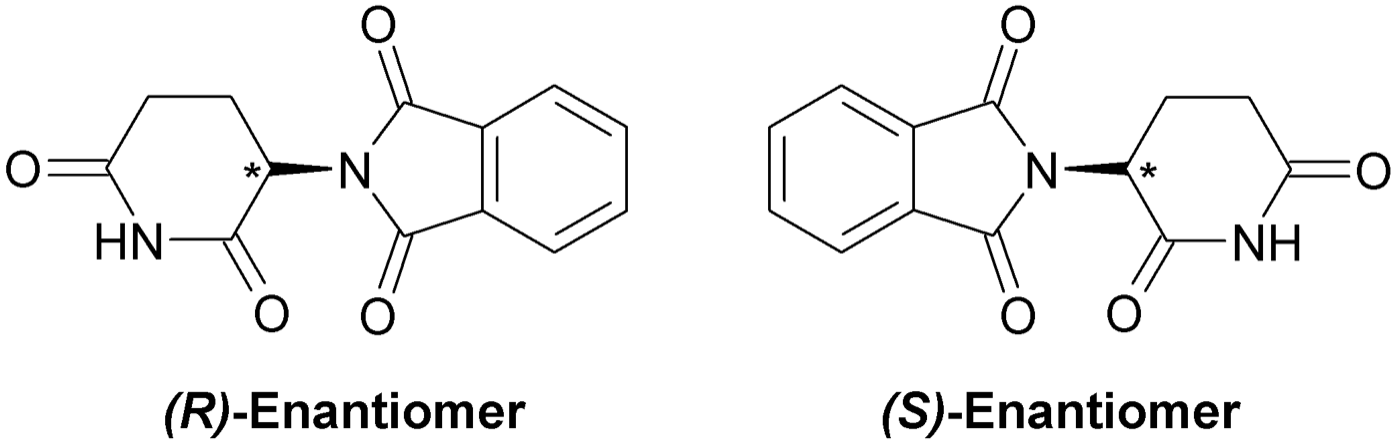
The reality is more sobering. The two forms of thalidomide interconvert inside the body — give a patient the "safe" enantiomer and it will partly turn into the other — so manufacturing a single pure form would not, in fact, have prevented the disaster. The deeper lesson is not about chirality at all but about teratogenicity: the drug crossed the placenta and interfered with the delicate molecular choreography of limb formation (modern work points to its binding of a protein called cereblon). The point that mattered in 1961, and that matters still, is simpler than the chemistry: the drug had never been tested for any of this, and the assumption that it was safe for the unborn was exactly that — an assumption, never a finding.
The fight for accountability
If the medical catastrophe was swift, the reckoning was agonisingly slow, and in many ways it remains unfinished. In Germany, a criminal prosecution of Grünenthal executives began in 1968, but the trial dragged on for over two years and ended in 1970 without verdicts; the proceedings were halted and the company agreed to pay into a compensation fund without any admission or finding of guilt. For the affected families it was a hollow outcome — the makers of the drug that had injured their children walked away uncondemned. Grünenthal did not issue a public apology until 2012, half a century after the withdrawal, and survivors widely regarded even that as too little, too late.
In Britain, the distributor Distillers at first offered the injured children meagre compensation, and the families faced a legal system stacked against them. The breakthrough came through journalism: in 1972 The Sunday Times, under the editor Harold Evans, mounted a campaign exposing the inadequacy of the settlement and the conduct behind the drug, fighting a legal injunction all the way — a battle that eventually reached the European Court of Human Rights and became a landmark for press freedom. Public pressure forced Distillers to greatly increase compensation, and a trust was established for the British thalidomide survivors. In Sweden, where the drug had been sold as Neurosedyn by Astra, affected families likewise organised and secured compensation. Everywhere, the survivors themselves — growing up, and then growing old, with the consequences — became the most powerful witnesses to what had been done.
Their lives are the part of the story that the word "compensation" never quite captures. The thalidomide survivors grew up learning to do with two or three fingers, or with feet where hands should have been, things the rest of the world does without thinking, and many built full lives — careers, families, advocacy — out of that difficulty. But the bodies that were altered before birth do not stop ageing, and survivors now in their sixties face compounding pain and wear that the original settlements, calculated decades ago, never anticipated. Some national survivor groups have had to fight a second and third time for adequate support. The disaster, in other words, did not end in 1961, or with any settlement; it is still being lived, every day, by the people it was inflicted on — which is the strongest possible argument that the protections it produced must never be allowed to erode.
What it changed
The thalidomide disaster did something few scandals do: it permanently changed the rules. Before thalidomide, drug regulation in much of the world was thin, and a manufacturer's assurance carried enormous weight. After it, that deference was gone.

In the United States, the near miss gave decisive momentum to a reform that had been stalled in Congress. The Kefauver-Harris Amendment of 1962, signed by President Kennedy, transformed the FDA's mandate: drug companies now had to demonstrate that a medicine was not only safe but effective, through adequate and well-controlled studies, before it could be marketed; adverse effects had to be reported; and patients in drug trials had to give informed consent. Kelsey, lately an obscure reviewer, was honoured by the President and became the public face of the principle that a regulator's job is to demand proof. Around the world, governments followed, building systems that required extensive testing — including, now, specific testing for effects on the fetus — before a drug could reach the public. The modern apparatus of drug approval, with all its slowness and all its caution, is in large part thalidomide's monument.
The drug that came back
There is a final, strange chapter. Thalidomide, the most infamous drug of the twentieth century, never entirely went away — and has since returned as a genuinely valuable medicine, under conditions of extraordinary control. In 1964 a doctor in Israel, Jacob Sheskin, gave thalidomide to a desperately suffering leprosy patient as a sedative and discovered that it dramatically relieved a painful complication of the disease. Decades later, researchers found it effective against multiple myeloma, a cancer of the blood, and against other conditions; its derivatives became important cancer drugs.
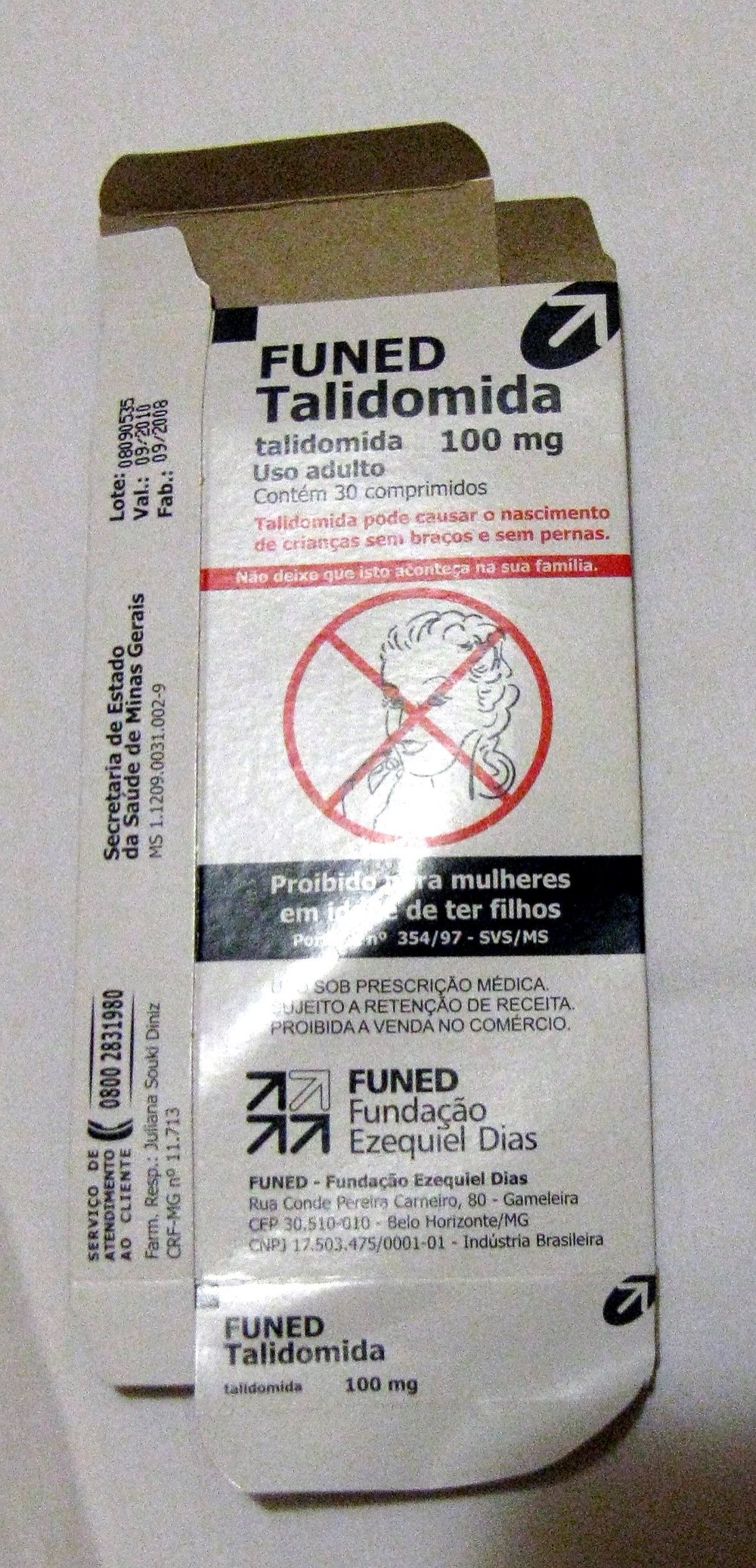
So thalidomide is prescribed again today — but hedged with the most stringent safeguards any drug carries. Patients and prescribers enrol in rigorous programmes; women of childbearing age must use reliable contraception and undergo pregnancy testing; the packaging, as in Brazil, screams its warning in symbol and text. The drug that became a byword for medical disaster is now also a case study in how a dangerous medicine can be used responsibly — precisely because the catastrophe it caused is never allowed to be forgotten. Its second life is built entirely on the memory of its first.
In the end, thalidomide is remembered for two opposite things at once: as one of the worst medical catastrophes ever inflicted on the innocent, and as the event that built the protections meant to ensure it never happens again. Both are true, and the link between them is the uncomfortable core of the story. The safeguards exist because the disaster happened; the disaster happened because the safeguards did not yet exist. A generation of children, born in the brief window when a drug could be sold as safe on nothing but a promise, are the reason that no drug, in most of the world, can be sold that way again. It is worth remembering what their lesson cost — and worth insisting that it stay learned.
Sources
- Frances Oldham Kelsey, FDA records and her account of the Kevadon (thalidomide) new-drug application review (1960–62) — primary.
- W. Lenz, contemporary medical reports linking thalidomide to congenital malformations (1961–62) — primary.
- W. G. McBride, letter to The Lancet on congenital abnormalities (December 1961) — primary.
- The Kefauver-Harris Drug Amendments of 1962 and the US legislative record — primary.
- The Sunday Times "Suffer the Children" investigation and Harold Evans's account of the thalidomide campaign (1970s) — secondary.
- Trent Stephens and Rock Brynner, Dark Remedy: The Impact of Thalidomide and Its Revival as a Vital Medicine (2001) — secondary.
- Records of the Contergan trial in Germany (1968–70) and the subsequent compensation foundation — primary.
- Histories of the thalidomide disaster and of drug regulation, including scholarship on the FDA and the 1962 amendments — academic.
- J. Sheskin and later clinical literature on thalidomide's use in leprosy (ENL) and multiple myeloma — academic.
- Accounts of the British, Swedish, and other national thalidomide survivor groups and compensation settlements — secondary.
Inspired this / based on it
Jacqui and David Morris
Documentary on the Sunday Times campaign for thalidomide survivors under editor Harold Evans.
Trent Stephens and Rock Brynner
Basic Books. A history of the disaster and the drug's unexpected return as a medicine.
The Sunday Times Insight Team
The landmark investigative account behind the British compensation campaign.
Filed under
- #thalidomide
- #neurosedyn
- #contergan
- #grunenthal
- #frances-kelsey
- #fda
- #pharmaceuticals
- #birth-defects
- #drug-regulation
- #1950s
- #1960s
- #confirmed
Click any tag for every article carrying it.
Continue reading
Purdue Pharma and OxyContin
In December 1995, the U.S. Food and Drug Administration approved a new extended-release oxycodone formulation manufactured by the privately-held Stamford, Connecticut pharmaceutical company Purdue Pharma. The drug was called OxyContin. Its FDA-approved label stated that the controlled-release formulation 'is believed to reduce the abuse liability of the drug.' Within weeks of the January 1996 launch, Purdue's sales force was telling physicians that the risk of addiction was 'less than one percent' — a number drawn from a single 1980 letter to the editor in the *New England Journal of Medicine* that the company would, over the next twenty years, cite approximately 600 times in its promotional materials. The letter had observed 4 cases of addiction in 11,882 hospitalized patients given any opioid for any duration. It was not, by any reasonable standard, evidence for an outpatient sustained-release formulation. By 2010, OxyContin's annual revenue had reached approximately $3.1 billion. By 2017, drug overdose was the leading cause of death for Americans under 50. The cumulative U.S. opioid death toll from 1999 to 2023, by the CDC's count, exceeded 700,000. Purdue Pharma pleaded guilty to federal criminal misbranding charges in 2007 (paying $634.5 million) and again in 2020 (agreeing to $8.3 billion in penalties as part of a bankruptcy reorganization). The Sackler family — owners of Purdue throughout the period — were the subject of a separate $6 billion settlement that was struck down by the U.S. Supreme Court in 2024 (*Harrington v. Purdue Pharma*) and is, as of mid-2026, being renegotiated. Patrick Radden Keefe's 2021 book *Empire of Pain* is the most comprehensive single-volume treatment of the case.

Big Tobacco's Cancer Cover-Up
On the morning of January 4, 1954, a full-page advertisement appeared in 448 American newspapers under the headline *A Frank Statement to Cigarette Smokers*. It was signed by the chief executives of the United States' six largest tobacco companies. The advertisement assured the American public that 'there is no proof that cigarette smoking is one of the causes of cancer' and that the industry would underwrite scientific research to find the truth. The advertisement had been drafted by John W. Hill of the Hill & Knowlton public-relations firm, hired by the tobacco industry's chief executives at a meeting at the Plaza Hotel in New York on December 14-15, 1953. The strategy that the meeting produced — manufacture doubt about epidemiological evidence the industry already privately accepted, do this through industry-funded research that produced findings inconsistent with the public-health consensus, and continue to sell cigarettes to American smokers while doing so — would be sustained for forty-four years. It would be ended, in 1998, by the Master Settlement Agreement: the largest civil legal settlement in American history at $206 billion across 25 years, paid by the surviving tobacco companies to 46 states, the District of Columbia, and five U.S. territories. By that point, an estimated 8 million Americans had died from smoking-related cancers, cardiovascular disease, and respiratory illness during the cover-up period.

The Vipeholm Experiments and the Toffee Made to Rot Teeth
At the Vipeholm hospital outside Lund, in southern Sweden, the patients could not leave and could not consent. They were adults with severe intellectual disabilities, classified in the language of the time as 'uneducable,' housed for life in a state institution that controlled every meal they ate. And in the years after the Second World War, that total control made them, in the eyes of Sweden's medical authorities, the perfect material for an experiment. The country had one of the worst rates of tooth decay in the world, and the National Board of Health wanted to understand, definitively, what caused it. So between 1945 and the mid-1950s, researchers used the people of Vipeholm to find out — feeding different groups different diets, and, in the most notorious phase, giving some of them large quantities of a specially formulated sticky toffee, eaten between meals, that was engineered to cling to the teeth and bathe them in sugar for as long as possible. The patients' mouths were the laboratory. Many of them developed severe, irreversible cavities. The studies that resulted were a genuine scientific landmark: they established, more clearly than any work before, that it is sugar — and above all sugar eaten frequently and in sticky form — that drives tooth decay. That finding reshaped dentistry and gave Sweden its enduring tradition of lördagsgodis, sweets saved for Saturdays. But it was bought with the teeth of people who were never asked, and could not have answered. This is the story of what was done at Vipeholm, what it taught the world, and the question it leaves about the price of knowledge.