
The National Palace of Guatemala in Guatemala City, photographed in 1948 — the period of the experiments. With the cooperation of the Guatemalan government, United States Public Health Service doctors used the country's prisons, army, and mental hospital as a laboratory for deliberately infecting people with sexually transmitted diseases. Wikimedia Commons / Janice Waltzer, CC BY 2.0.
The Guatemala Syphilis Experiments and the Deliberate Infection of the Powerless
Guatemala, 1946–1948 — United States government doctors deliberately infected more than a thousand prisoners, soldiers, psychiatric patients, and sex workers with syphilis and other diseases, without their consent, to test penicillin. It stayed hidden for over sixty years
- Category
- Health & Medicine
- Published
- Length
- 4,360 words · 19 min read
- Author
- The editors
The Guatemala syphilis experiments are, even among the dark episodes in this archive, unusually stark. There is no ambiguity about what happened, no contested verdict, no plausible defence. United States government doctors deliberately infected vulnerable people with serious diseases, without their consent, in a foreign country chosen because it offered subjects who could not say no. The only mystery the story holds is how it stayed secret for so long — and what it says that it could happen at all, carried out by respectable physicians who knew, even then, that it was wrong.
This is the story of that crime and its long silence.
The men behind it
The Guatemala experiments did not come from nowhere. They grew out of a genuine wartime and post-war problem: sexually transmitted diseases, especially syphilis, were a serious threat to soldiers and to public health, and the recent arrival of penicillin raised an urgent question. Penicillin could cure syphilis — but could it also prevent it, given soon after exposure, as a prophylaxis? Answering that meant knowing precisely when someone had been infected, which is hard to study in the real world, where exposure is unpredictable. The researchers' solution was to control the exposure themselves: to infect people deliberately, at a known moment, and then test whether the drug could stop the disease from taking hold.
The question was a serious one, and the people asking it were not fringe figures. Syphilis had been a scourge for centuries, and the United States had waged a major public-health campaign against it, led by a Surgeon General who had made venereal disease a national priority. Penicillin, which had only just become widely available, had transformed the outlook almost overnight — a few injections could cure an infection that had once meant a lifetime of suffering — and the prospect that it might also prevent infection was genuinely important, with obvious value for a military that lost enormous numbers of man-days to STDs. None of that justifies what was done. But it matters for understanding it: the Guatemala experiments were not the work of cranks or sadists at the margins of medicine. They were authorised, funded, and staffed by the mainstream of American public health, pursuing a real scientific question by monstrous means.
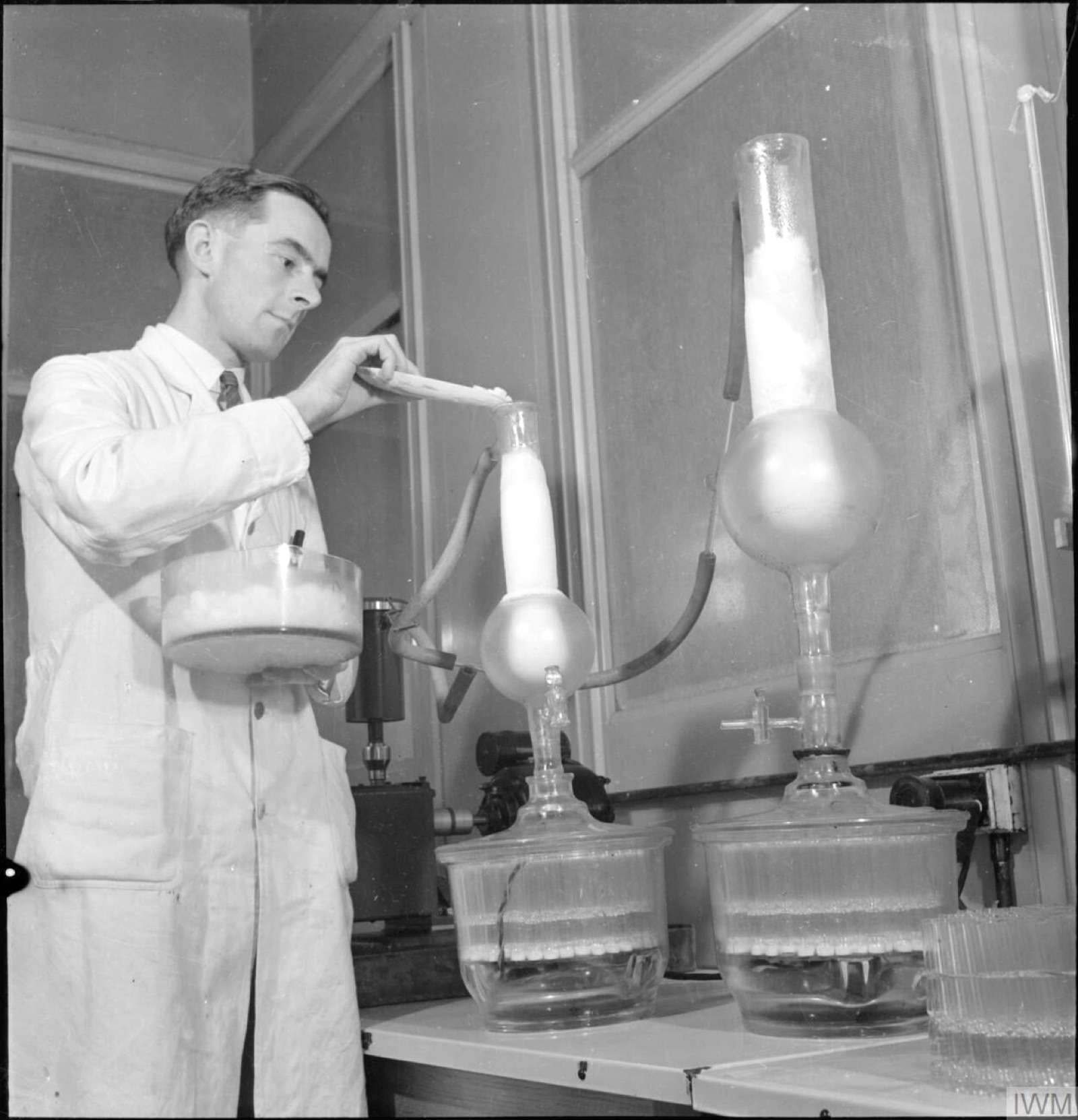
The work was run by the United States Public Health Service and funded through a grant from the National Institutes of Health, with the cooperation of senior figures in American medicine, including the Surgeon General. The physician in day-to-day charge was Dr John Charles Cutler, a PHS officer, working with Guatemalan health officials and the Pan American Sanitary Bureau. The choice of Guatemala was deliberate and practical: the country's government was willing to cooperate, and its institutions — prisons, the army, the national mental hospital — held captive populations whose exposure the researchers could control completely, in a setting where American rules and American scrutiny did not reach. It was, in the plainest terms, a place where they could do what they could not do at home.
The wider context made such an arrangement easy to imagine. The United States in the 1940s exercised enormous influence over Central America, where its government and corporations — the United Fruit Company foremost among them — treated countries like Guatemala almost as economic dependencies. American doctors and institutions moved through the region with the confidence of people operating in their own sphere of influence, and a research programme that required the cooperation of a friendly local government and access to its captive institutions fit naturally into that relationship. The Guatemalan officials who agreed to host the work, including doctors in its own health service, were participants in it; the disregard for the subjects' humanity was not solely an American import. But the power, the funding, the design, and the purpose were American, and so was the calculation that what happened to poor Guatemalans in a prison or an asylum would never trouble anyone who mattered.
The method
What was done to the subjects is difficult to read, and it should be, because softening it would be a second dishonesty. The researchers began by trying to spread the diseases "naturally": they arranged for commercial sex workers, some already infected and some deliberately infected for the purpose, to have sex with male prisoners, in order to transmit syphilis and gonorrhea. When this did not produce enough infections to study, they turned to direct methods. They abraded the skin of the genitals, or other parts of the body, and applied the bacteria directly; they introduced infectious material into the eyes, the mouth, and by injection; in some cases they inoculated the diseases by spinal puncture. Among the people infected this way were patients at the national psychiatric hospital — men and women with serious mental illness who could not possibly have understood what was being done to them or agreed to it.

Throughout, the defining feature was the absence of consent. The subjects were not meaningfully informed of the purpose; they were not asked whether they were willing; in many cases they did not know they were being infected at all, and some were led to believe they were receiving treatment rather than disease. The whole design depended on the subjects' inability to refuse — on the fact that prisoners, conscripts, and asylum patients in 1940s Guatemala were simply not in a position to say no. After infecting them, the researchers tested penicillin and other agents to see whether the diseases could be prevented or cured, and drew blood repeatedly to study the body's response. Not everyone who was infected was even reliably treated afterward.

A great deal of the work, in fact, was about the blood tests themselves. One of the study's stated aims was to evaluate and improve the serological tests used to diagnose syphilis — the laboratory methods that detect the body's response to infection — and this required drawing and analysing blood from large numbers of people whose true infection status was known because the researchers had controlled it. So the subjects were bled repeatedly, their samples shipped and studied, in a programme that treated several thousand human beings as a convenient supply of standardised, infected blood. The deliberate infections were the most shocking part of the Guatemala work, but the casual, large-scale use of people's bodies for testing ran through all of it.
Why Guatemala
It is worth dwelling on why the experiments happened where they did, because the choice of Guatemala was not incidental but central. The same researchers had, around the same time, conducted a related study on prisoners in Terre Haute, Indiana — but there they had used volunteers, men who agreed to take part, because in the United States the norms of consent, however thin, could not simply be ignored, and deliberately infecting unconsenting Americans was unthinkable. In Guatemala, those constraints fell away. A cooperative government, a population with no power and no recourse, and the distance from American oversight together created a space where the researchers could do what would have been impossible at home.

This is the logic of the whole affair, and it is worth naming plainly: the experiments were an export of unethical research to a place where the people harmed would not, and could not, object. It is the same pattern that recurs whenever the powerful conduct on the vulnerable, and especially the foreign and the poor, what they would never dare conduct on themselves. The Guatemalans infected with syphilis were not participants in a shared scientific endeavour. They were a resource, selected because they were available and because their suffering would be invisible.
Buried
For all the effort, the experiments produced little of scientific value. The data on penicillin prophylaxis were inconclusive, the methods were a mess, and the results were never published in any medical journal. But the deeper reason the work vanished was that those involved understood, at some level, that it could not bear the light. Cutler's superiors worried about how it would look; the safest course was silence. The records were not destroyed, but they were not shared either — they were simply filed away among Cutler's personal papers, and there they sat for decades, as he went on with a long career in public health.
That career included, in the years that followed, a central role in the study for which Cutler is most infamous: the Tuskegee syphilis study in Alabama, in which the Public Health Service observed hundreds of Black American men with syphilis for decades while deliberately leaving them untreated. The continuity is not a coincidence. The same institution, and in part the same people, treated the Black poor of Alabama and the captive poor of Guatemala as legitimate subjects for experiments that the comfortable and the powerful would never have tolerated being performed on themselves or their own.
What makes the buried record so chilling is precisely that nothing forced it into the open. Tuskegee ended in 1972 only because a whistleblower leaked it to the press; Guatemala had no whistleblower at all. Cutler kept his files, retired, and died in 2003 with his Guatemala work still unknown to the public, his reputation intact, an emeritus professor of a respected school of public health. Had his papers been discarded, or had no historian thought to read them closely, the experiments would simply have ceased to exist as a known fact — a thousand people deliberately infected, and not a trace in the public memory. The silence was not the failure of the cover-up. The silence was the cover-up, and it very nearly worked completely.
The discovery
The Guatemala experiments might have stayed buried indefinitely had they not crossed the path of a scholar studying their notorious sibling. Susan Reverby, a historian at Wellesley College and a leading authority on the Tuskegee study, was working through John Cutler's archived papers when she came upon documents describing something she had never heard of: not the passive observation of Tuskegee, but the active, deliberate infection of people in Guatemala. She recognised what she was looking at, and in 2010 she brought it to light.
The reaction was swift and, by the standards of historical reckonings, remarkably high-level. In October 2010, President Barack Obama personally telephoned the president of Guatemala to apologise; Secretary of State Hillary Clinton and the Secretary of Health and Human Services issued a joint statement calling the experiments "clearly unethical" and "reprehensible." Obama ordered a presidential bioethics commission to investigate. The United States government, in other words, did not deny or minimise what Reverby had found. It confirmed it, and condemned it, in the clearest terms.
That candour is, in its way, the one creditable thread in the whole story, and it is worth marking. Governments rarely confess so quickly or so completely to historical crimes, especially ones that had been safely forgotten and that no living official had committed. The United States could have minimised the disclosure, quibbled over details, or let it fade; instead it confirmed the findings at the highest level and ordered an unsparing investigation of itself. The acknowledgement does not undo the harm, and the absence of compensation that followed shows the sharp limit of what an apology accomplishes. But the contrast with the original silence is instructive. The crime depended on darkness; once the documents were in the open, the wrong was so plain that not even the government responsible tried to defend it. The difference between 1948 and 2010 was not that the act became wrong. It was that it became visible.
The reckoning
In 2011 the Presidential Commission for the Study of Bioethical Issues published its report, with the unsparing title Ethically Impossible. It laid out the experiments in detail and reached a conclusion that matters greatly: the researchers had violated ethical standards that existed at the time — that this was not a case of judging the past by the standards of the present. The proof was in their own conduct. The same scientists had used consenting volunteers in their Indiana study; they plainly understood that consent existed and mattered, and they deliberately withheld it in Guatemala because they knew the subjects there would never have agreed. They knew, and they did it anyway, and they hid it. That is not the innocence of a less enlightened age. It is guilt.
The apology and the report, however, did not bring justice to the people harmed. Guatemalan victims and their descendants sued the United States government, but the courts dismissed the case on the grounds of sovereign immunity — the government generally cannot be sued for such acts committed abroad. The victims then turned to the institutions and companies they alleged had helped design, fund, or supply the research; that litigation has ground on for years. As of the most recent developments, the people deliberately infected in Guatemala, or the families of those who died, had received apologies and condemnation but no meaningful compensation. The reckoning, such as it was, remained largely symbolic.
The lawsuits are worth understanding, because they show how hard it is to convert even an admitted wrong into redress. When the suit against the United States government was thrown out on sovereign immunity, the victims' lawyers turned to private defendants — including a major university whose doctors had been involved in designing or reviewing the work, a large philanthropic foundation, and a pharmaceutical company that had supplied materials — arguing that these institutions bore responsibility for a programme they had helped make possible. The defendants fought hard to have the case dismissed, but a federal judge allowed key claims to proceed, meaning that, decades on, the question of institutional liability for the Guatemala experiments is still being litigated in American courts. For the elderly survivors and the descendants of the dead in Guatemala, it has been a slow, uncertain process conducted in a foreign legal system, with no guarantee of anything at the end of it. An apology can be delivered in an afternoon. Justice, it turns out, is far harder to arrange.
What is established, and what it means
There is nothing factually unresolved about the Guatemala experiments. They happened; the documents are explicit; the United States government itself has confirmed and condemned them. What the case offers is not a mystery to solve but a truth to confront — about consent, about the use of the powerless, and about the way that unethical research has historically flowed toward those least able to refuse it.
It would be comfortable to file Guatemala away as an aberration, a single bad actor in John Cutler operating in a less careful age. The presidential commission's findings make that consolation impossible. This was a Public Health Service operation, funded by the nation's premier medical research body, known to senior figures, and conducted by people who understood consent well enough to seek it elsewhere and withhold it here. It belongs to a pattern — running through [[tuskegee-syphilis]], through the use of prisoners and institutionalised people as subjects, through the whole history of medicine practised on the poor and the captive rather than with them — in which the bodies of the powerless were treated as a commons for science. Guatemala is the pattern in its most naked form: not the withholding of treatment, but the active giving of disease, to people chosen because they could not say no.
In the end, the Guatemala syphilis experiments are a study in what becomes possible when consent is treated as optional for some people and not others. The doctors who carried them out were not monsters in any cinematic sense; they were professionals who had simply decided, or absorbed from the world around them, that the prisoners and patients of a poor foreign country did not have the standing to be asked. They infected them, studied them, and moved on, confident enough that no one would ever know. For sixty years they were right. That the truth surfaced at all is owed to an archive and a historian, not to any conscience among those involved — and the lesson is that a crime can be complete, documented, and entirely successful in its silence, and still be a crime. The people of Guatemala were owed a choice. They were given a disease instead.
Sources
- Presidential Commission for the Study of Bioethical Issues, "Ethically Impossible": STD Research in Guatemala from 1946 to 1948 (2011) — primary.
- Susan M. Reverby, "'Normal Exposure' and Inoculation Syphilis: A PHS 'Tuskegee' Doctor in Guatemala, 1946–48," Journal of Policy History (2011) — academic.
- The archived papers of Dr John C. Cutler (University of Pittsburgh) documenting the Guatemala experiments — primary.
- Joint statement of Secretary of State Hillary Clinton and HHS Secretary Kathleen Sebelius, and the US apology to Guatemala (October 2010) — primary.
- Court records of the Guatemalan victims' lawsuits against the United States government and against institutions and companies (2011 onward) — primary.
- Susan M. Reverby, Examining Tuskegee: The Infamous Syphilis Study and Its Legacy (2009) — academic, for the Tuskegee connection.
- Reporting by The New York Times, the Associated Press, and others on the 2010 disclosure and its aftermath — secondary.
- Government of Guatemala's own inquiry into the experiments — primary.
- Histories of human-subjects research ethics and the Nuremberg Code (1947) — academic.
Inspired this / based on it
US Presidential Commission for the Study of Bioethical Issues
The official report that documented and condemned the experiments after their 2010 discovery.
Susan M. Reverby
By the historian who uncovered the Guatemala records while studying the related Tuskegee study.
Filed under
- #guatemala-syphilis
- #guatemala
- #public-health-service
- #john-cutler
- #human-experimentation
- #informed-consent
- #syphilis
- #medical-ethics
- #1940s
- #confirmed
Click any tag for every article carrying it.
Continue reading

The Tuskegee Syphilis Study
In 1932, the U.S. Public Health Service began a study of 399 Black men in Macon County, Alabama, who had syphilis. They were told they were being treated. They were not. For forty years — including the twenty-five years after penicillin became standard care — the Public Health Service watched the disease take its course. A whistleblower's documents reached the Associated Press on July 25, 1972, and the study ended a few months later. President Clinton apologized on behalf of the United States government in 1997.
Henrietta Lacks and the Cells That Would Not Die
In the early months of 1951, a thirty-one-year-old Black woman named Henrietta Lacks went to the Johns Hopkins Hospital in Baltimore — one of the few hospitals in the segregated United States that would treat Black patients — with a cervical cancer that was killing her with frightening speed. During her treatment, a surgeon shaved two small samples from her cervix, one healthy and one cancerous, and sent them to a laboratory down the hall. No one asked Henrietta's permission, and no one told her; this was simply how things were done, especially to a poor Black patient in a charity ward. She died that October and was buried in an unmarked grave. But the cancer cells from that sample did something no human cells had ever reliably done before: they survived, and divided, and kept dividing, doubling every day, apparently without limit. They were the first immortal human cell line, and the scientist who grew them named them HeLa, after the first letters of her first and last names. Over the following decades those cells — descended from a woman almost no one knew anything about — would become one of the foundational tools of modern biology: used to develop the polio vaccine, to map the human genome, to test drugs and radiation and cosmetics, to study cancer and AIDS and the viruses that cause them, sent into space, and grown by the ton and sold around the world in a multi-billion-dollar industry. Henrietta's own family knew none of it for more than twenty years, received nothing, and in many cases could not afford the medicine her cells helped create. This is the story of the woman behind HeLa, of what was taken and what was built from it, and of a debt that the science of an era was structured never to pay.

The Vipeholm Experiments and the Toffee Made to Rot Teeth
At the Vipeholm hospital outside Lund, in southern Sweden, the patients could not leave and could not consent. They were adults with severe intellectual disabilities, classified in the language of the time as 'uneducable,' housed for life in a state institution that controlled every meal they ate. And in the years after the Second World War, that total control made them, in the eyes of Sweden's medical authorities, the perfect material for an experiment. The country had one of the worst rates of tooth decay in the world, and the National Board of Health wanted to understand, definitively, what caused it. So between 1945 and the mid-1950s, researchers used the people of Vipeholm to find out — feeding different groups different diets, and, in the most notorious phase, giving some of them large quantities of a specially formulated sticky toffee, eaten between meals, that was engineered to cling to the teeth and bathe them in sugar for as long as possible. The patients' mouths were the laboratory. Many of them developed severe, irreversible cavities. The studies that resulted were a genuine scientific landmark: they established, more clearly than any work before, that it is sugar — and above all sugar eaten frequently and in sticky form — that drives tooth decay. That finding reshaped dentistry and gave Sweden its enduring tradition of lördagsgodis, sweets saved for Saturdays. But it was bought with the teeth of people who were never asked, and could not have answered. This is the story of what was done at Vipeholm, what it taught the world, and the question it leaves about the price of knowledge.